THIS POST AND THE ONE BEFORE WILL BE OUT OF SYNC. THE REASON IS THAT A COMMENT WAS POSTED (SPAM) THAT HAD NOTHING TO DO WITH THIS BLOG'S TOPIC, NEITHER WAS IT POSTED BY ANYONE I KNEW. THE ONLY WAY I COULD REMOVE IT WAS TO DELETE THE WHOLE POST. I'M SORRY FOR ANY CONFUSION THIS MAY CAUSE. I HOPE YOU CAN STILL UNDERSTAND WHAT I'M TRYING TO SAY IN THE INFORMATION.
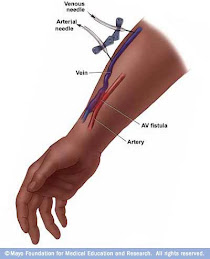
This first illustration (BELOW)shows the catherter which is a temporary solution to an emergency situation.
The arm access is an AV fistula. An AV fistula is the gold standard for vascular access for hemodialysis and is associated with the lowest failure and complication rates when compared with other forms of vascular access.
An AV fistula requires advance planning because a fistula takes a while after surgery to develop But a properly formed fistula is less likely than other kinds of vascular accesses to form clots or become infected. Also, fistulas tend to last many years, longer than any other kind of vascular access.
A surgeon creates an AV fistula by connecting an artery directly to a vein, usually in the forearm. Connecting the artery to the vein causes more blood to flow into the vein. As a result, the vein grows larger and stronger, making repeated insertions for hemodialysis treatments easier.
Arteriovenous Graft
If you have small veins that won't develop properly into a fistula, you can get a vascular access that uses a synthetic tube implanted under the skin in your arm. The tube becomes an artificial vein that can be used repeatedly for needle placement and blood access during hemodialysis. A graft doesn't need to develop as a fistula does, so it can be used sooner after placement, often within 2 or 3 weeks.
Compared with fistulas, grafts tend to have more problems with clotting or infection and need replacement sooner, but a well-cared-for graft can last for several years.
There are other options that I won't explore here. There are plenty of sites to find all you might want to know. I hope this might clear up any confusion you might have about dialysis.